Pyloric stenosis is a condition that affects young babies, usually between birth and five months of age. It happens when the muscle around the pylorus — the passage between the stomach and the small intestine — thickens and narrows over time. This blockage makes it very hard for milk or formula to move through, causing forceful vomiting after feedings. In this article, we explain what pyloric stenosis is, how to spot it early, and what treatment looks like for Canadian families.
What Is Pyloric Stenosis?
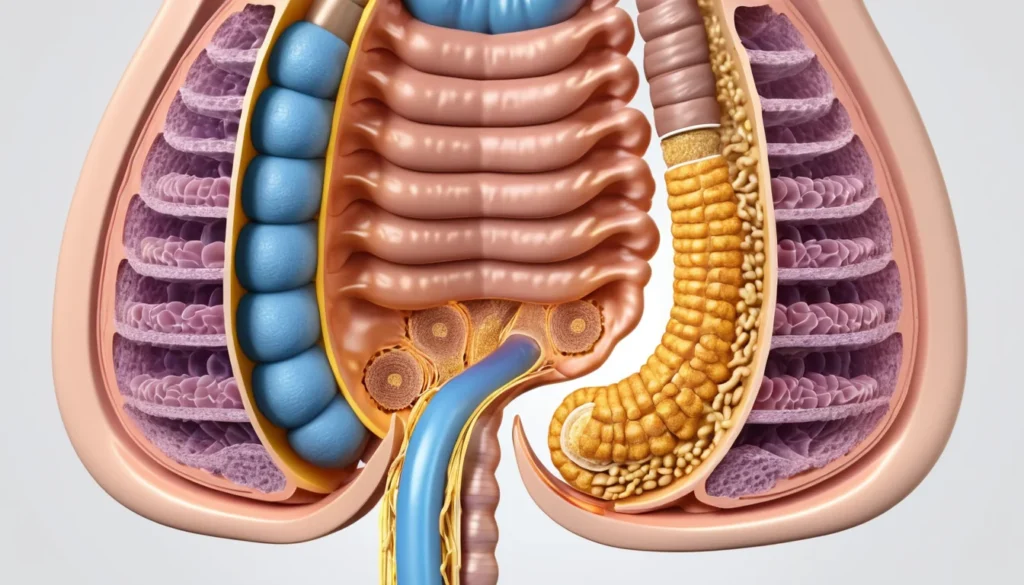
The pylorus is a small muscular valve at the bottom of the stomach. It controls the flow of food from the stomach into the first part of the small intestine, called the duodenum. In babies with pyloric stenosis, this valve becomes thickened and too narrow to let food pass through properly.
Most cases develop around three weeks of age. However, symptoms can appear anytime from birth up to five months. Premature babies may show signs a little later than full-term newborns.
For more background on infant digestive conditions, visit Health Canada’s official health resource centre.
What Causes Pyloric Stenosis?
Doctors do not know the exact cause of pyloric stenosis. However, research points to several factors that may play a role.
Genetics: A family history of pyloric stenosis increases a baby’s risk. If a parent had the condition, their child is more likely to develop it.
Antibiotic use: Some studies suggest that giving newborns erythromycin — an antibiotic — in the first two weeks of life may be linked to a higher risk. That said, most babies with pyloric stenosis were never given this medication.
Sex: It is about four times more common in baby boys than in girls.
Birth order: First-born children appear to be at slightly higher risk.
In the past, doctors believed pyloric stenosis was present at birth. Current evidence strongly suggests it develops after birth, as the muscle gradually thickens over the first few weeks of life.
Recognising the Symptoms of Pyloric Stenosis
The most obvious sign of pyloric stenosis is forceful vomiting after feeding. This is often called “projectile vomiting” because the milk can shoot out with surprising force. It is different from normal baby spitting up, which is gentle and small in volume.
Symptoms tend to start mild and get worse over days or weeks. As the pylorus becomes narrower, vomiting becomes more frequent and more powerful. According to Mayo Clinic’s guide on pyloric stenosis, parents should watch for a clear pattern of worsening vomiting.
Common Symptoms to Watch For
Vomiting shortly after most feedings — breast milk or formula only, not yellow or green
Visible swelling in the upper abdomen after eating
Constant hunger, even right after vomiting
Irritability and fussiness that does not settle
Fewer bowel movements than usual, or harder stools
Fewer wet diapers, which signals dehydration
Poor weight gain or actual weight loss
Becoming increasingly sleepy or lethargic
As dehydration sets in, a baby may become less alert and harder to wake. This is a serious sign that requires immediate medical attention.
When to See a Doctor
You should contact your family doctor or visit a walk-in clinic right away if your baby shows any of these warning signs:
Vomits most of the milk at two or more feedings in a row
Vomit is yellow or green in colour — this can signal a more serious problem
Shows signs of dehydration (fewer wet diapers, dry mouth, sunken eyes)
Loses weight or stops gaining weight
Is unusually sleepy or difficult to wake
If your regular family doctor is unavailable, a walk-in clinic can assess your baby quickly. Many provincial health plans across Canada — including those in Ontario, British Columbia, and Alberta — cover urgent paediatric visits. If your baby seems very unwell, go directly to the nearest hospital emergency department. Do not wait.
Always speak with a healthcare professional for a proper diagnosis. This article is for general information only and is not a substitute for medical advice.
How Is Pyloric Stenosis Diagnosed?
A doctor will begin by taking a full health history and doing a physical exam. During the exam, they may be able to feel a small, firm lump — about the size of an olive — in your baby’s upper abdomen. This lump is the thickened pyloric muscle.
The doctor may also observe wave-like movements across the baby’s stomach after a feeding. These are the stomach muscles working hard to push food through the narrowed opening.
Diagnostic Tests
Two main tests confirm pyloric stenosis:
Abdominal ultrasound: This is the most common and preferred test. It uses sound waves to create an image of the pylorus and can clearly show if the muscle is too thick.
Upper GI endoscopy: In some cases, a small camera is passed into the digestive tract to get a closer look. This is less common for initial diagnosis.
Blood tests are also done to check for dehydration and electrolyte imbalances, which are common in babies who have been vomiting frequently. Correcting these imbalances is an important step before any surgery takes place.
Treatment for Pyloric Stenosis
The only effective treatment for pyloric stenosis is surgery. The procedure is called a pyloromyotomy. The good news is that once this surgery is done, the condition does not come back. Most children recover fully and go on to feed and grow normally.
Preparing for Surgery
Surgery is not usually performed immediately after diagnosis. If the baby is dehydrated, doctors will first give fluids through an intravenous (IV) line for 24 to 48 hours. A small tube may be placed through the nose and into the stomach to drain fluid and relieve pressure. This preparation is important for the baby’s safety during the operation.
Types of Pyloromyotomy
There are two ways to perform the procedure. The surgical team will decide which is most appropriate for your baby.
Open surgery: The surgeon makes a small cut in the abdomen. The thickened pyloric muscle is then carefully split — but not removed — to widen the passage. This allows food to flow through properly again.
Laparoscopic surgery: The surgeon inserts a tiny camera (called a laparoscope) through a small cut near the belly button. A few additional small cuts allow the surgeon to complete the same muscle-splitting procedure. This minimally invasive approach often results in a faster recovery and less visible scarring.
Both methods are safe and widely available at children’s hospitals and major medical centres across Canada. Your paediatric surgeon will explain which option is best suited to your child.
Recovery After Surgery
After the operation, your baby will receive clear fluids first, followed by breast milk or formula within 24 hours. Most babies are ready to go home within two days of surgery.
It is normal for babies to vomit a small amount in the first day or two after the operation. However, if vomiting continues after discharge or becomes frequent again, contact your doctor promptly. This could mean the muscle was not fully divided during surgery, which is rare but treatable.
Post-operative complications are uncommon. The most frequent issue is a minor infection at the incision site. Signs include redness, swelling, or discharge around the cut. If you notice any of these, see your family doctor or visit a walk-in clinic as soon as possible.
Caring for Your Baby at Home
Once home, feed your baby small amounts more frequently rather than large feedings at once. This helps the healing stomach adjust. Parents should feel comfortable holding, cuddling, and playing with their baby as normal. Bonding and skin-to-skin contact remain just as important during recovery.
If you have concerns at any stage, do not hesitate to call your family doctor or your province’s health information line — such as Ontario’s Telehealth Ontario or BC’s 8-1-1 HealthLink BC service. These services offer free health advice from registered nurses any time of day.
For additional guidance on infant health and nutrition, Healthline’s overview of pyloric stenosis offers helpful parent-friendly information.
Frequently Asked Questions About Pyloric Stenosis
How do I know if my baby has pyloric stenosis or just normal spitting up?
Normal baby spitting up is gentle and involves small amounts of milk. Pyloric stenosis causes forceful, projectile vomiting that shoots out with significant force and involves most of the feeding. If vomiting is getting worse over several days and your baby seems hungry right after vomiting, speak with your family doctor as soon as possible.
At what age does pyloric stenosis usually start?
Pyloric stenosis most commonly develops around three weeks of age, though it can appear anytime between birth and five months. Premature babies may show symptoms a little later. The condition rarely appears after five months of age.
Is pyloric stenosis surgery dangerous for babies?
Pyloromyotomy — the surgery used to treat pyloric stenosis — is considered a routine and very safe procedure when performed at a paediatric surgery centre. Serious complications are rare. Most babies recover quickly and are eating normally within 24 hours of surgery.
Can pyloric stenosis come back after surgery?
No. Once a pyloromyotomy is performed to treat pyloric stenosis, the condition does not return. The surgery permanently widens the passage between the stomach and the intestine. Your child will not need any further treatment for this condition.
Is pyloric stenosis covered by provincial health plans in Canada?
Yes. Diagnosis and surgical treatment for pyloric stenosis are medically necessary procedures covered under provincial and territorial health insurance plans across Canada. This includes hospital stays, surgery, and follow-up care. Contact your provincial health authority if you have questions about your specific coverage.
What is the difference between open surgery and laparoscopic surgery for pyloric stenosis?
Both procedures correct pyloric stenosis by splitting the thickened pyloric muscle. Open surgery uses a slightly larger incision on the abdomen, while laparoscopic surgery uses a tiny camera inserted near the belly button and requires only very small cuts. Laparoscopic surgery often means a faster recovery and less scarring, but your surgeon will recommend the best option for your baby.
Key Takeaways
Pyloric stenosis is a narrowing of the passage between a baby’s stomach and small intestine, causing forceful vomiting.
It most often develops around three weeks of age and can occur up to five months.
The main symptom is projectile vomiting after most feedings, which gets worse over time.
Dehydration and weight loss are serious signs that need immediate medical attention.
Diagnosis is confirmed with an ultrasound and physical examination.
The only treatment is a safe surgical procedure called a pyloromyotomy. It is fully covered under Canadian provincial health plans.
Recovery is fast. Most babies are home within two days and feeding normally soon after.
If you are concerned about your baby’s vomiting, contact your family doctor, visit a walk-in clinic, or call your province’s health information line right away.