Adenomyosis is a uterine condition where the tissue that normally lines the inside of the uterus grows into the muscular wall of the uterus itself. This can cause heavy periods, severe cramping, and chronic pelvic pain. Many Canadian women live with adenomyosis without knowing it, because symptoms can be mild or easy to dismiss. This article explains what adenomyosis is, who it affects, and what your treatment options look like.
What Is Adenomyosis?
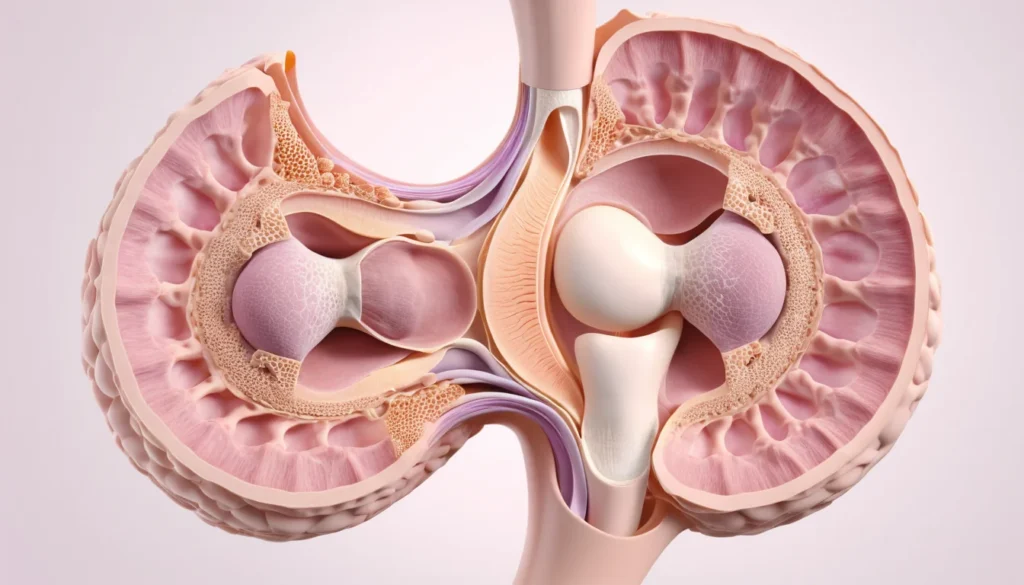
Your uterus has two main layers. The inner layer is called the endometrium — a thin, soft lining. The outer layer is muscle, called the myometrium. In adenomyosis, endometrial tissue pushes through and grows inside the muscle layer.
This displaced tissue still behaves like normal endometrial tissue. It thickens and bleeds with every menstrual cycle. However, because the blood has nowhere to go, it causes inflammation, pain, and an enlarged uterus.
The good news is that adenomyosis is not cancer and does not increase your risk of cancer. In addition, it often resolves on its own after menopause, when oestrogen levels drop significantly.
How Common Is Adenomyosis?
Adenomyosis is more common than many people think. Because it is often symptom-free, many cases go undiagnosed and unreported, making it difficult to know the exact numbers.
Research suggests that adenomyosis is more frequent in women over 40, and in those who have had uterine surgery. However, recent studies show it is also rising among younger women and teenagers.
Approximately 2% to 5% of teenagers who experience painful periods may have adenomyosis. For more background on uterine health conditions, Mayo Clinic’s overview of adenomyosis is a reliable starting point.
Signs and Symptoms of Adenomyosis
Many women with adenomyosis have no symptoms at all. Others experience symptoms that significantly affect their daily lives. The range and severity vary from person to person.
Common Symptoms to Watch For
Heavy menstrual bleeding — soaking through pads or tampons quickly
Prolonged periods — bleeding that lasts longer than usual
Severe menstrual cramps (dysmenorrhea) — cramping that is worse than typical period pain
Chronic pelvic pain — ongoing discomfort outside of your period
Painful intercourse (dyspareunia)
Worse-than-usual premenstrual syndrome (PMS)
Because the uterus can enlarge with adenomyosis, some women feel a sense of pressure, bloating, or heaviness in the lower abdomen. You may not see the enlargement, but you may feel it.
Could It Be Something Else?
Adenomyosis shares symptoms with other uterine conditions, such as fibroids, endometriosis, and uterine polyps. Therefore, it is important to get a proper medical assessment rather than self-diagnosing. A family doctor or walk-in clinic can help you start the process.
What Causes Adenomyosis?
The exact cause of adenomyosis is not yet known. However, researchers have proposed several theories based on what they observe in patients.
Leading Theories
Invasive tissue growth. Some researchers believe endometrial cells invade the muscle wall directly. Uterine incisions — such as those made during a C-section — may make this easier.
Developmental origin. Others suggest that endometrial tissue is deposited abnormally in the muscle wall during fetal development, making adenomyosis a congenital condition.
Post-childbirth inflammation. After labour and delivery, the uterus becomes inflamed. This may disrupt the boundary between the endometrium and the muscle layer.
Stem cell involvement. A newer theory suggests that bone marrow stem cells may invade the myometrium and trigger adenomyosis.
Regardless of how it starts, adenomyosis is known to be influenced by oestrogen. The condition tends to worsen during the reproductive years and improve after menopause, when oestrogen levels fall.
Risk Factors for Adenomyosis
Certain factors appear to increase the likelihood of developing adenomyosis or experiencing noticeable symptoms. These include:
Previous uterine surgery, including C-sections, fibroid removal, or surgical abortion
A history of childbirth and labour
Being between the ages of 40 and 50
Long-term exposure to oestrogen over a lifetime
Most diagnosed cases are found in women approaching menopause. However, this does not mean younger women are immune. Rates among younger women and adolescents are increasing, according to recent research from Healthline’s adenomyosis resource.
Possible Complications
Adenomyosis itself is not life-threatening. However, if left unmanaged, it can lead to complications that affect your health and quality of life.
Chronic Anaemia
Heavy, prolonged menstrual bleeding can lead to chronic anaemia — a condition where your body does not have enough healthy red blood cells. Anaemia causes fatigue, weakness, dizziness, and can make it harder for your body to function well overall.
Impact on Daily Life
Ongoing pelvic pain and heavy bleeding can interfere with work, exercise, relationships, and activities you enjoy. Dysmenorrhea is not something you should simply push through. It deserves proper medical attention and treatment.
If you are missing days of work or school because of your period, that is a sign something needs to be addressed. Your provincial health plan covers visits to a family doctor or walk-in clinic, so do not hesitate to seek help.
How Is Adenomyosis Diagnosed?
Diagnosing adenomyosis can be challenging because its symptoms overlap with other conditions. Your doctor will typically rule out fibroids, endometriosis, and polyps before suspecting adenomyosis.
Diagnostic Tools Your Doctor May Use
Pelvic exam — to check for an enlarged or tender uterus
Ultrasound — a common, non-invasive first step
MRI (Magnetic Resonance Imaging) — provides a more detailed image of the uterine walls
Endometrial biopsy — occasionally used to rule out other conditions
It is worth knowing that a definitive diagnosis of adenomyosis can only be confirmed by examining uterine tissue after a hysterectomy (surgical removal of the uterus). In practice, however, most doctors diagnose and treat it based on symptoms and imaging results.
When to See a Doctor
You should speak with a healthcare provider if you experience any of the following:
Periods that are unusually heavy or last longer than seven days
Severe cramping that does not respond to over-the-counter pain relievers
Pelvic pain that continues outside of your period
Pain during sex
Fatigue that may be linked to blood loss
Remember: painful periods are not normal. They are common, but not something you have to accept. Start by booking an appointment with your family doctor or visiting a walk-in clinic. They can refer you to a gynaecologist if needed. Health Canada also encourages Canadians to seek care early for menstrual health concerns — do not wait for symptoms to worsen.
Treatment Options for Adenomyosis
The right treatment for adenomyosis depends on your age, symptoms, and whether you plan to have children in the future. The condition improves naturally after menopause, so treatment for women close to menopause may focus on managing symptoms rather than curing the condition.
Non-Surgical Options
Anti-inflammatory medications (NSAIDs) — such as ibuprofen, taken before and during your period to reduce pain and bleeding
Hormonal therapy — birth control pills, hormonal IUDs, or progestin therapy can reduce or stop menstrual bleeding and ease pain
GnRH agonists — medications that temporarily induce a menopause-like state to reduce symptoms; usually short-term due to side effects
Surgical Options
Uterine artery embolization — a minimally invasive procedure that cuts off blood supply to the affected tissue
Endometrial ablation — destroys the uterine lining; suitable for women who do not wish to become pregnant
Hysterectomy — the only permanent cure for adenomyosis; recommended only when other treatments have failed and the patient does not want future pregnancies
Your doctor will guide you through the options that best fit your situation. For a broader look at uterine health treatments, the WHO fact sheet on endometriosis and related conditions offers helpful global context. Always consult your doctor before starting or stopping any treatment.
Frequently Asked Questions About Adenomyosis
Can adenomyosis go away on its own?
Adenomyosis often improves significantly after menopause, when oestrogen levels in the body decline. However, it does not typically resolve on its own during the reproductive years. Treatment can help manage symptoms effectively in the meantime.
Is adenomyosis the same as endometriosis?
No — they are related but different conditions. In endometriosis, tissue similar to the uterine lining grows outside the uterus. In adenomyosis, that tissue grows within the uterine muscle wall itself. Some women have both conditions at the same time.
Can you get pregnant if you have adenomyosis?
Many women with adenomyosis do conceive and carry pregnancies successfully. However, adenomyosis may make it more difficult to get pregnant in some cases. If you are trying to conceive and have been diagnosed with adenomyosis, speak with your doctor or a fertility specialist.
How is adenomyosis different from uterine fibroids?
Fibroids are non-cancerous growths that form on or within the uterus as distinct lumps. Adenomyosis, by contrast, involves endometrial tissue dispersed throughout the uterine muscle with no distinct mass. Both can cause heavy bleeding and pelvic pain, which is why proper diagnosis matters.
Does adenomyosis increase the risk of cancer?
Adenomyosis is a benign (non-cancerous) condition and is not considered a risk factor for uterine cancer. However, because symptoms overlap with other conditions, it is always important to get a thorough evaluation from your doctor to rule out other causes.
Is adenomyosis covered under Canadian provincial health plans?
In Canada, visits to a family doctor, gynaecologist referrals, and diagnostic imaging such as ultrasound and MRI are generally covered under provincial health plans. Treatment costs vary depending on your province and the specific procedures involved. Check with your provincial health authority for details specific to your coverage.
Key Takeaways
Adenomyosis occurs when uterine lining tissue grows into the uterine muscle, causing heavy bleeding, cramping, and pelvic pain.
It is more common in women over 40 but can affect younger women and teenagers too.
Many women have adenomyosis without any symptoms and never know it.
Painful, heavy periods are not something you have to accept — they deserve medical attention.
Treatment ranges from hormonal therapy and anti-inflammatory medications to surgery, depending on your needs.
Adenomyosis typically improves after menopause as oestrogen levels decline.
Start by speaking with your family doctor or visiting a walk-in clinic — your provincial health plan covers these visits.
Always consult a qualified healthcare provider before making decisions about your treatment.